
Libido and Erectile Dysfunction on Steroids
Why Steroid-Related Sexual Dysfunction Is Not One Problem
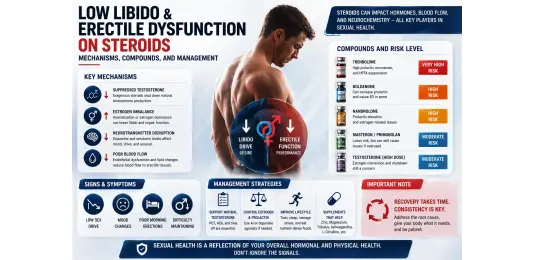
Sexual dysfunction during or after a steroid cycle is one of the most reported — and most poorly managed — adverse effects in performance pharmacology. The reason for the poor management is straightforward: athletes and their advisors frequently treat all steroid-related ED and low libido as a single phenomenon requiring a single response. In reality, steroid-related sexual dysfunction has at least four distinct hormonal mechanisms, each requiring a different intervention, and applying the wrong intervention can worsen the problem.
The four primary mechanisms:
- Prolactin elevation — from progestogenic compounds (Nandrolone, Trenbolone); dopamine antagonist effect suppresses libido and impairs erectile function
- Estrogen imbalance — both excessive estrogen (water retention, desensitisation) and insufficient estrogen (AI over-suppression, collagen impairment, psychological effects) impair sexual function through different pathways
- HPTA suppression and low testosterone — on-cycle from 19-nor compounds' extreme suppression without testosterone base; post-cycle from the lag between compound clearance and endogenous testosterone recovery
- Psychological contributors — anxiety, mood disturbance, and sleep disruption from the cycle compounds themselves, which inhibit sexual function independently of hormonal mechanism
The psychological dimension — particularly relevant during Trenbolone cycles with their characteristic mood and anxiety profile — is covered at Psychological Effects of Steroids. This article focuses on the hormonal mechanisms and their pharmacological management.
"Deca Dick": Nandrolone and Prolactin-Driven Sexual Dysfunction
"Deca Dick" is the colloquial term for the pattern of libido suppression and erectile dysfunction associated with Nandrolone-based compound use — and it is the most pharmacologically predictable form of steroid-related sexual dysfunction. The mechanism involves two parallel pathways:
- Prolactin elevation: Nandrolone's progestogenic activity stimulates pituitary prolactin secretion. Elevated prolactin directly suppresses hypothalamic GnRH pulsatility, reducing LH and endogenous testosterone — but more relevantly for sexual function, prolactin has a direct inhibitory effect on dopaminergic tone in the limbic system. Dopamine is the primary driver of sexual motivation. Elevated prolactin blunts the dopaminergic signal responsible for libido, producing the characteristic low-desire, low-responsiveness sexual presentation. The full prolactin management framework is at Prolactin on Steroids: Control.
- DHT displacement: Nandrolone and its metabolite dihydronandrolone compete with testosterone for 5-alpha reductase, reducing systemic conversion to DHT. Since DHT is a critical driver of sexual function and penile tissue androgen sensitivity, reduced DHT availability in the absence of supplemental testosterone impairs erectile function and tactile sexual response.
The consistent management protocol for Nandrolone-containing cycles: always run with a testosterone base (minimum 200–250 mg/week) to maintain systemic testosterone and DHT availability, and use Cabergoline prophylactically from the first injection to prevent prolactin elevation before it develops. "Deca Dick" is almost entirely preventable with this approach — it is primarily a problem for athletes who run Nandrolone without these supports.
Trenbolone, Prolactin, and Libido Suppression
Trenbolone compounds produce prolactin-driven sexual dysfunction through the same progestogenic mechanism as Nandrolone, but typically with faster onset and potentially greater severity at performance doses. The combination of prolactin elevation, dopaminergic disruption, and the neurological side effects unique to Trenbolone — covered at Trenbolone Side Effects — creates a compound profile where libido impairment is frequent and requires active management from cycle initiation rather than a reactive response to emerging symptoms.
Cabergoline is the primary management agent for prolactin-driven sexual dysfunction from both Nandrolone and Trenbolone. Dosing at 0.25–0.5 mg twice weekly, calibrated by prolactin bloodwork, is the standard approach. Where prolactin is managed and sexual dysfunction persists on Trenbolone, the psychological and neurological mechanisms — not a hormonal deficit — are likely the primary remaining driver.
Estrogen Imbalance: Both Too High and Too Low
Estrogen's role in male sexual function is substantially more important than the performance community typically acknowledges. At physiological levels, estrogen modulates nitric oxide signalling in penile vascular endothelium, supports libido through central receptor activity, and contributes to normal erectile response. Both extremes impair function:
- Excessive estrogen: Very high estradiol from high-dose testosterone cycles without aromatase inhibitor use produces water retention, gynecomastia risk, and emotional/mood changes — but also contributes directly to sexual dysfunction through estrogenic over-activation of negative feedback pathways and progesterone receptor cross-activation. The symptom presentation includes reduced libido with preserved erectile function, emotional sensitivity, and the estrogenic physical changes. This is the scenario where appropriate AI use (calibrated AI dose, not maximum AI dose) is the correct intervention.
- Insufficient estrogen (AI over-suppression): Driving estradiol below 15–20 pg/mL with aggressive AI dosing produces its own form of sexual dysfunction — often more severe and harder to recognise as iatrogenic (AI-caused). Symptoms: severely reduced libido, difficulty achieving or maintaining erection, emotional flatness, and joint pain simultaneously. This is among the most common misdiagnosed sexual dysfunction scenarios in performance pharmacology — the athlete blames the anabolic compounds, increases AI dose believing estrogen is still the problem, and worsens the dysfunction further. The intervention is AI dose reduction until estradiol returns to the 20–35 pg/mL range, confirmed by bloodwork.
Post-Cycle Testosterone Crash: The Libido Trough
The most temporally predictable form of steroid-related sexual dysfunction is the post-cycle libido crash — the period after exogenous compound clearance when endogenous testosterone has not yet recovered. With both testosterone and estradiol at their nadir, sexual desire, erectile function, and arousal capacity are all significantly impaired.
This phase is inseparable from the HPTA recovery process detailed at HPTA Suppression on Steroids. Correctly timed PCT using Clomiphene Tablets and Tamoxifen Tablets — which stimulate LH and FSH production — shortens this trough significantly by restoring endogenous testosterone faster. Athletes who skip PCT or start it incorrectly timed typically experience a 2–4 month post-cycle libido trough rather than the 3–6 week window achievable with structured PCT.
PDE5 Inhibitors: Sildenafil and Tadalafil on Cycle
Phosphodiesterase-5 inhibitors (PDE5i) — Sildenafil and Tadalafil — address the erectile function component of sexual dysfunction through a vascular mechanism that operates independently of hormonal cause. They inhibit the PDE5 enzyme in penile vascular smooth muscle, prolonging cGMP-mediated vasodilation and facilitating erection in response to sexual stimulation. They do not restore libido (desire) — they address the mechanical erectile component only.
- Sildabol Tablets (Sildenafil, British Dragon) — the fast-acting PDE5 inhibitor, taken 30–60 minutes before activity, with a 4–6 hour window. Effective for on-demand use when erectile function is the primary complaint on cycle.
- Taldabol Tablets (Tadalafil, British Dragon) — the longer-acting PDE5 inhibitor with a 36-hour window. Can be taken at a daily low dose (2.5–5 mg) for continuous vascular support, or at 10–20 mg for on-demand use. The extended half-life makes Tadalafil particularly useful during cycles where erectile dysfunction is persistent rather than situational.
PDE5 inhibitors have meaningful utility during steroid cycles but do not resolve the hormonal causes of sexual dysfunction — they provide symptomatic support while the underlying hormonal issue is identified and addressed. An athlete with prolactin-driven libido collapse will not experience restored desire from Sildenafil or Tadalafil; they will experience improved erectile mechanics in a context of unchanged desire. Cabergoline addresses the desire component; PDE5 inhibitors address the mechanics.
PT-141: Central Mechanism Libido Support
PT-141 (Bremelanotide) is a melanocortin receptor agonist that operates through a central neurological mechanism entirely distinct from PDE5 inhibitors. Where Sildenafil and Tadalafil work peripherally in penile vascular tissue, PT-141 activates melanocortin receptors (MC3R and MC4R) in the hypothalamus and limbic system, directly stimulating dopaminergic pathways associated with sexual desire and arousal — the central neurological component that PDE5 inhibitors do not address.
PT-141 is therefore complementary to PDE5 inhibitors rather than an alternative. In contexts where both libido (desire) and erectile function are impaired — the typical presentation of prolactin elevation or severe post-cycle testosterone crash — PT-141 addresses the central desire component while Tadalafil or Sildenafil addresses the peripheral erectile component. Standard dosing: 1–2 mg subcutaneous injection 45–90 minutes before activity. Side effects at standard doses: transient facial flushing, mild nausea (most common in the first 1–2 uses, typically diminishing with subsequent use).
Preventing Sexual Dysfunction: Getting the Hormonal Environment Right
- Always run testosterone base with 19-nor compounds: Nandrolone or Trenbolone without a testosterone base is the most reliable route to "Deca Dick" — minimum 200 mg/week testosterone from any ester maintains baseline sexual function while the Nandrolone component is managed with Cabergoline
- Calibrate AI dosing to bloodwork, not symptoms: Targeting estradiol 20–35 pg/mL based on actual bloodwork prevents both estrogen excess and AI-driven estrogen deficiency sexual dysfunction — the two most easily preventable causes of cycle-related ED
- Begin Cabergoline prophylactically on any progestogenic cycle: Prolactin should be managed before symptoms appear — waiting for libido collapse to begin Cabergoline is managing established dysfunction rather than preventing it
- Start PCT at the correct time: Ester-specific PCT timing that minimises the post-cycle testosterone trough is the primary tool for reducing the duration and severity of post-cycle libido suppression
Conclusion
Sexual dysfunction on steroids has specific causes with specific solutions. Prolactin from Nandrolone or Trenbolone: Cabergoline. Estrogen excess: calibrated AI use. Estrogen deficiency from AI over-suppression: AI dose reduction confirmed by bloodwork. Post-cycle testosterone trough: correctly timed PCT. For symptomatic relief of erectile dysfunction while hormonal causes are addressed: Sildabol Tablets (Sildenafil) or Taldabol Tablets (Tadalafil) manage the mechanical component. For central libido restoration: PT-141 addresses the dopaminergic desire pathway that PDE5 inhibitors do not reach. None of these tools are substitutes for correct hormonal management — they are bridges while the root cause is resolved.
FAQ
Q1. What exactly is "Deca Dick" and how does Nandrolone cause it?
"Deca Dick" describes the pattern of libido suppression and erectile dysfunction specifically associated with Nandrolone-based compounds — Decabol 250 (Nandrolone Decanoate) and Durabol 100 (Nandrolone Phenylpropionate). The two parallel mechanisms: elevated prolactin from Nandrolone's progestogenic activity suppresses dopaminergic libido drive through the hypothalamic-pituitary pathway; and Nandrolone's competition with testosterone for 5-alpha reductase reduces systemic DHT availability, impairing the penile androgenic signalling that supports erectile response. Running Nandrolone without a testosterone base compounds both mechanisms by eliminating the remaining testosterone and DHT source. The solution: testosterone base at minimum 200 mg/week, Cabergoline prophylactically from day one. Deca Dick is almost entirely preventable. Q2. Can I use Sildenafil or Tadalafil during a steroid cycle?
Yes — Sildabol Tablets (Sildenafil) and Taldabol Tablets (Tadalafil) are safe to use during a steroid cycle in athletes without contraindicated cardiovascular conditions. PDE5 inhibitors work through a peripheral vascular mechanism that is independent of the androgenic or hormonal activity of the cycle compounds. The primary interaction to be aware of: PDE5 inhibitors and nitrate compounds (including amyl nitrite/poppers) produce severe hypotension and must not be combined. Both agents are appropriate for symptomatic ED management on cycle while the hormonal cause is being identified and addressed. Tadalafil at low daily doses (2.5–5 mg/day) is also of interest for its cardiovascular effects on nitric oxide signalling, independent of sexual function support. Q3. Will libido return to normal after the cycle ends?
In the majority of athletes who run correctly structured post-cycle therapy, libido returns to pre-cycle baseline within 6–12 weeks of completing PCT. The timeline depends on cycle length, suppression severity, and PCT effectiveness — details covered at HPTA Suppression on Steroids. Athletes who experience persistent libido impairment beyond 12 weeks post-PCT should investigate with a complete hormonal panel: total testosterone, free testosterone, LH, FSH, estradiol, and prolactin. Persistent elevation of prolactin post-cycle (from very long Nandrolone or Trenbolone cycles) can maintain libido suppression beyond the testosterone recovery timeline and may require ongoing Cabergoline use into the post-cycle period. Q4. What is PT-141 and how does it help with steroid-related low libido?
PT-141 (Bremelanotide) is a melanocortin receptor agonist that works centrally in the brain — activating MC3R and MC4R receptors in the hypothalamus and limbic system to stimulate the dopaminergic pathways associated with sexual desire. Unlike PDE5 inhibitors (Sildenafil, Tadalafil) which address peripheral erectile mechanics, PT-141 directly stimulates sexual motivation and desire at the neurological level. This makes it specifically useful in contexts where desire is the primary complaint — prolactin-driven libido suppression, post-cycle dopaminergic flatness, or the psychological/CNS component of sexual dysfunction. Standard dosing is 1–2 mg subcutaneous injection 45–90 minutes before activity. Most commonly reported side effects are transient facial flushing and mild nausea, typically diminishing after the first few uses. Q5. How do I know whether my ED is from estrogen, prolactin, or testosterone?
The presentations differ in ways that allow reasonable differential diagnosis before bloodwork, though bloodwork is the only reliable confirmation. Estrogen excess: ED accompanied by water retention, emotional sensitivity, nipple sensitivity, bloating — the full estrogenic side effect picture. Estrogen deficiency from AI over-suppression: ED with joint pain, emotional flatness, low motivation, and absence of estrogenic symptoms despite a testosterone-based cycle — the estrogen crash picture described at Psychological Effects of Steroids. Prolactin elevation: low desire (libido collapse) disproportionate to erectile mechanics, accompanied by possible nipple sensitivity unrelated to estrogen, occurring on a Nandrolone or Trenbolone cycle. Post-cycle testosterone crash: low desire and poor erectile function appearing after compound clearance, resolving progressively during PCT. Bloodwork: estradiol, prolactin, total and free testosterone, LH, and FSH will confirm the mechanism.